Page last updated: May 2024
The information on this webpage was adapted from Understanding Bladder Cancer - A guide for people with cancer, their families and friends (2024 edition). This webpage was last updated in May 2024.
Expert content reviewers:
This information was developed based on international clinical practice guidelines, and with the help of a range of health professionals and people affected by bladder cancer:
- Dr Prassannah Satasivam, Urologist and Robotic Surgeon, Epworth Hospitals and Cabrini Hospitals, VIC
- Donna Clifford, Urology Nurse Practitioner, Royal Adelaide Hospital, SA
- Marc Diocera, Genitourinary Nurse Consultant, Peter MacCallum Cancer Centre, VIC
- Dr Renee Finnigan, Radiation Oncologist, Gold Coast University Hospital, QLD
- Lisa Hann, 13 11 20 Consultant, Cancer Council SA
- Dr Andrew Hirschhorn, Director of Allied Health and MQ Health Academy, MQ Health, Macquarie University, NSW
- Anne Marie Lyons, Stomal Therapy Nurse, Concord Hospital and NSW Stoma Limited, NSW
- John McDonald, Consumer
- Prof Manish Patel, Urological Cancer and Robotic Surgeon, Westmead Hospital, Macquarie University Hospital, and The University of Sydney, NSW
- Dr Jason Paterdis, Urological Surgeon, Brisbane Urology Clinic, QLD
- Graeme Sissing, Consumer
- Prof Martin Stockler, Medical Oncologist, The University of Sydney, Concord Cancer Centre, and Chris O’Brien Lifehouse RPA, NSW
Types of urinary diversions
If you have surgery to remove the bladder (radical cystectomy), you will need another way to collect and store urine. This is known as a urinary diversion. It is a major change, and your treatment team will offer support to help you adjust.
Your surgeon will talk to you about the best type of urinary diversion for your situation. They will recommend one of the following options:
- urostomy – creates a new opening to your urinary system
- neobladder – creates a new bladder from your small bowel
- continent urinary diversion – creates a pouch from your small bowel to hold urine until you are ready to drain it.
Urostomy
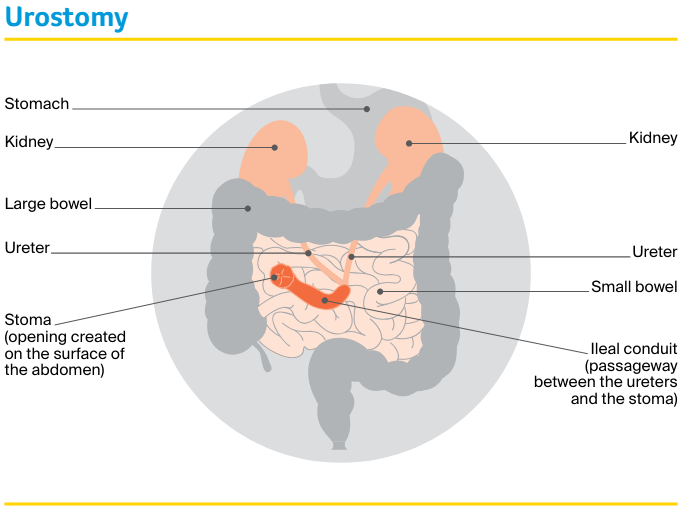
This is the most common type of urinary diversion. Also known as an ileal conduit, a urostomy means that urine will drain into a bag attached to the outside of the abdomen.
The surgeon will use a piece of your small bowel (ileum) to create a passageway (conduit). This connects the ureters (the tubes that carry urine from your kidneys) to an opening created on the surface of the abdomen called a stoma.
A watertight, drainable bag is placed over the stoma to collect urine. This small bag, worn under clothing, fills continuously and needs to be emptied throughout the day through a tap or bung on the bag.
The small bag will be connected to a larger drainage bag at night if required.
Positioning the stoma
Before the operation, the surgeon and/or a stomal therapy nurse will plan where the stoma will go. They will discuss the position with you and aim to place the stoma so it doesn’t move when you sit, stand or move.
Sometimes the position can be tailored for particular needs. For example, golfers may prefer the stoma to be placed so that it doesn’t interfere with their golf swing.
The stoma will usually be created on the abdomen, to the right of the bellybutton.
Having a stoma
For the first few days after the operation, the stomal therapy nurse will look after the stoma and make sure the bag is emptied and changed as often as necessary.
Once you are ready, the stomal therapy nurse will teach you and/or your carer/family member how to care for the stoma.
At first, the stoma will be slightly swollen and it may be several weeks before it settles down. The stoma may also produce a thick, white substance (mucus), which might appear as pale threads in the urine.
The amount of mucus will lessen over time, but it won’t disappear completely.
Stents (small plastic tubes) will be used to help with the flow of urine while the ureters heal. These stents are placed at the time of surgery and are temporary.
They will be removed before you are discharged from hospital, or up to 3 weeks after surgery. Your surgeon will talk to you about when the stents will be removed.
Attaching the bag – There are different types of bags (sometimes called appliances) and the stomal therapy nurse will help you choose one that suits you. The nurse will show you how to clean your stoma and change the bags.
This will need to be done regularly, usually every day while in hospital (for teaching purposes) and every 2–3 days after that. It might be helpful to have a close relative or friend join you when the nurse gives the instructions so they can support you at home.
Emptying the bag – How often you need to empty a bag is affected by how much you drink. Staying hydrated is very important with a urostomy.
The first few times you empty the bag, allow yourself plenty of time and privacy so that you can work at your own pace without any interruptions.
Living with a stoma
Having a urostomy is a major change and many people feel overwhelmed at first. It’s natural to worry about how the urostomy will affect your appearance, lifestyle and relationships.
Learning to look after the urostomy may take time and patience. It may sometimes affect your travel plans and social life in the early days while you are gaining confidence, but these issues can be managed with planning.
After you learn how to take care of the stoma, you will find you can still do your regular activities.
You may worry about how the bag will look under clothing. Although the urostomy may seem obvious to you, most people won’t know you are wearing a bag unless you tell them about it.
Modern bags are usually flat and shouldn’t be noticeable under clothing.
After bladder surgery, you may have some physical changes that affect your sex life. You may worry about being rejected or having sex with your partner.
If you meet a new partner during or after treatment, it can be difficult to talk about your experiences, particularly if your sexuality and body image have been affected. Sexual intimacy may feel awkward at first, but open communication usually helps.
Many people find that once they talk about their fears, their partner is understanding and supportive, and they can work together to make sexual activities more comfortable.
Support for people with a stoma
Speaking to a counsellor or cancer nurse about your feelings and experiences can be helpful.
See a stomal therapy nurse – Stomal therapy nurses are trained in helping people with stomas. They will:
- arrange for you to speak with another person living with a stoma
- answer your questions about the surgery and side effects, including the impact on sexual activities and intimacy
- help you adjust to having a stoma and regain your confidence
- assist you with fitting and using urostomy bags
- give you written instructions on caring for your stoma
- provide ongoing care and support once you are home.
Stomal therapy nurses work in many hospitals. Before discharge, the nurse will make sure that you feel comfortable changing the urostomy bag and that you have a supply of bags.
If your hospital doesn’t have a stomal therapy nurse, your treatment team can help you find one. Or you may be able to find a nurse near you by visiting the Australian Association of Stomal Therapy Nurses.
Your doctor may also be able to arrange for a community nurse to visit you.
Join a stoma association – Your stomal therapy nurse will usually help you join a stoma association. For a small annual fee, you will be able to get support, free bags and related products. Visit the Australian Council of Stoma Associations.
Register for the Stoma Appliance Scheme – The Australian Government’s Stoma Appliance Scheme (SAS) provides free stoma bags and related products to people who have a stoma. To be eligible, you must have a Medicare card and belong to a stoma association.
“Having a stoma hasn’t been a problem. On the rare occasion the bag has leaked, it’s because I haven’t fitted it properly or changed it soon enough.” David
Managing stomas
Having a stoma, even temporarily, is a big change in a person’s life and takes some getting used to. However, thousands of Australians have a stoma and most lead a relatively normal life.
Call Cancer Council 13 11 20, or visit My Cancer Guide, to find local support services available to help manage your stoma.
Find services in your area
Neobladder
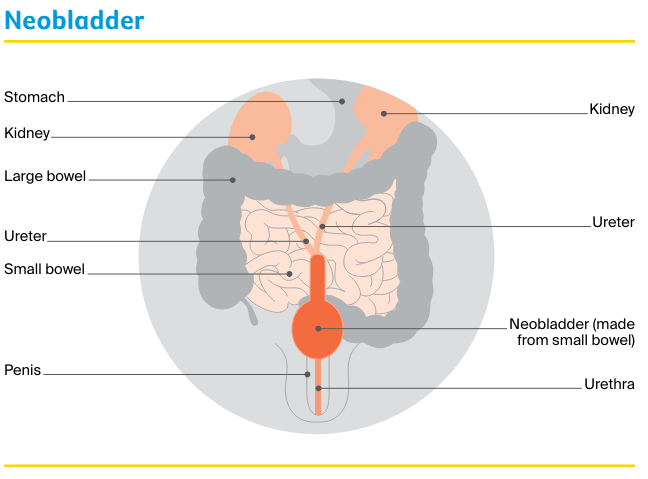
In this method, a pouch is created from a portion of your small bowel and placed in the same area as your original bladder. This pouch is called a neobladder.
The procedure for creating a neobladder is more complex and takes longer than creating a urostomy. However, you don’t need to have a stoma with a neobladder.
Once the neobladder is created, the surgeon will stitch it into the ureters to collect and store urine from the kidneys.
It will also be stitched into the urethra to drain urine from the body. The neobladder will allow you to urinate through your urethra, but it will feel different from urinating with a normal bladder.
“I couldn’t control the number of urinary tract infections after my surgery, but once I started catheterising, it limited the infections.” Mark
Living with a neobladder
It takes time to get used to a new bladder. The neobladder will not have the nerves that tell you when your bladder is full, and you will have to learn new ways to empty it.
The neobladder may produce a thick white substance (mucus), which might appear as pale threads in the urine. The amount of mucus will lessen over time, but it won’t disappear completely.
At first, the new bladder won’t be able to hold as much urine and you will probably need to empty your bladder every 2–3 hours. This will gradually increase to 4–6 hours, but it may take several months.
During that time the neobladder may leak when full, and you may have to get up during the night to go to the toilet.
Discuss any concerns with your nurse, physiotherapist, GP or urologist, and arrange follow-up visits with them. You may also find the following support useful:
- See a continence nurse or a pelvic floor physiotherapist – they will work with you to develop a toilet schedule to train your new bladder. Strengthening the pelvic floor muscles before and after surgery will help you control the neobladder. It can sometimes be difficult to fully empty the neobladder using your pelvic floor muscles, so the nurse may also teach you how to drain the bladder with a catheter. This is called intermittent self-catheterisation and it should usually be done twice a day to reduce the risk of urinary tract infections.
- Ask about the Continence Aids Payment Scheme (CAPS) – this scheme is operated by Services Australia (Medicare) and provides a payment for eligible people needing a long-term supply of continence aids, including catheters for draining the bladder. Ask the continence nurse if you’re eligible.
- Contact the National Continence Helpline – to speak to a nurse continence specialist.
BEAT Bladder Cancer Australia
BEAT Bladder Cancer Australia is a charity that raises awareness about bladder cancer.
It also provides information and support to people with bladder cancer and their carers, including videos, information sheets and question lists.
Learn more
Continent urinary diversion
In this procedure, the surgeon uses a piece of the small bowel to create a pouch inside the body. The pouch is designed so that it does not leak urine, but can be drained by inserting a catheter through a stoma.
Several times a day you will need to drain the urine by inserting a drainage tube (catheter) through the stoma into the pouch. This diversion procedure is not commonly used, but may be an option.
Your surgeon or nurse will explain the risks and benefits of this procedure, and how to empty urine from the pouch.
Life after bladder cancer
For most people, the cancer experience doesn’t end on the last day of treatment. Life after cancer treatment can present its own challenges.
It is important to allow yourself time to adjust to the physical and emotional changes, and establish a new daily routine at your own pace. Your family and friends may also need time to adjust.
Follow-up appointments
You will have regular appointments to monitor your health, manage any ongoing side effects and check that the cancer hasn’t come back or spread. How often you see your doctor will depend on the cancer type and treatments.
People who still have a bladder will have regular follow-up cystoscopies, as this is the best way to find bladder cancer that has come back.
The cystoscopy may be done in hospital in the outpatient department under local anaesthetic or in an operating theatre under general anaesthetic.
Depending on the stage and grade of the bladder cancer you had, you will need a follow-up cystoscopy every 3–12 months. This may continue for several years or for the rest of your life, but will become less frequent over time.
Between follow-up appointments, let your doctor know immediately of any symptoms or health problems.
What if bladder cancer returns?
Sometimes bladder cancer does come back after treatment, which is known as a recurrence. If the cancer recurs and you still have a bladder, the cancer can usually be removed while it is still in the early stages.
This will require a cystoscopy under general anaesthetic. If this isn’t possible, your doctor may consider removal of the bladder (cystectomy).
Some people need other types of treatment, such as chemotherapy, immunotherapy or radiation therapy. The treatment you have will depend on the stage, grade and risk category of the cancer, your previous treatment and your preferences.
