Page last updated: May 2024
The information on this webpage was adapted from Understanding Bladder Cancer - A guide for people with cancer, their families and friends (2024 edition). This webpage was last updated in May 2024.
Expert content reviewers:
This information was developed based on international clinical practice guidelines, and with the help of a range of health professionals and people affected by bladder cancer:
- Dr Prassannah Satasivam, Urologist and Robotic Surgeon, Epworth Hospitals and Cabrini Hospitals, VIC
- Donna Clifford, Urology Nurse Practitioner, Royal Adelaide Hospital, SA
- Marc Diocera, Genitourinary Nurse Consultant, Peter MacCallum Cancer Centre, VIC
- Dr Renee Finnigan, Radiation Oncologist, Gold Coast University Hospital, QLD
- Lisa Hann, 13 11 20 Consultant, Cancer Council SA
- Dr Andrew Hirschhorn, Director of Allied Health and MQ Health Academy, MQ Health, Macquarie University, NSW
- Anne Marie Lyons, Stomal Therapy Nurse, Concord Hospital and NSW Stoma Limited, NSW
- John McDonald, Consumer
- Prof Manish Patel, Urological Cancer and Robotic Surgeon, Westmead Hospital, Macquarie University Hospital, and The University of Sydney, NSW
- Dr Jason Paterdis, Urological Surgeon, Brisbane Urology Clinic, QLD
- Graeme Sissing, Consumer
- Prof Martin Stockler, Medical Oncologist, The University of Sydney, Concord Cancer Centre, and Chris O’Brien Lifehouse RPA, NSW
Bladder cancer begins when cells in the lining of the bladder (urothelium) become abnormal. This causes the cells to grow and divide out of control. As the cancer grows, it may start to spread into the deeper layers of the bladder wall.
Some cancer cells can also break off and travel outside the bladder to other parts of the body (e.g. lymph nodes, lungs, bones or liver).
The bladder
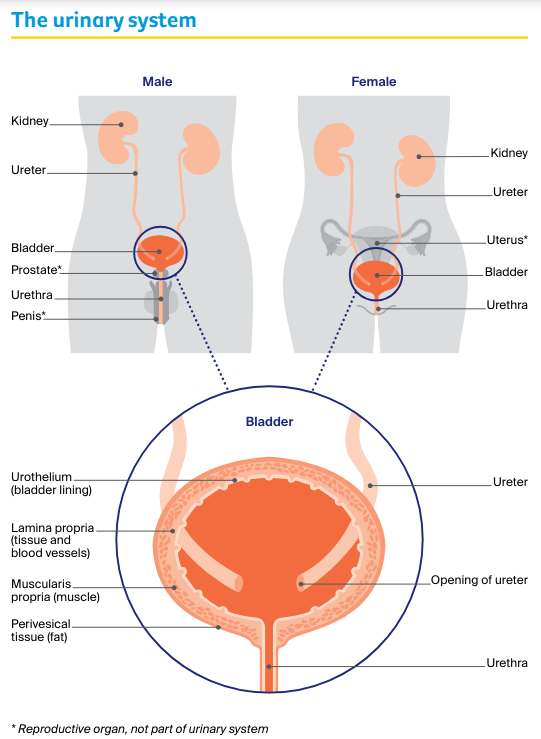
The bladder is a hollow, muscular sac that stores urine (wee or pee). It sits behind the pubic bone in the pelvis, and is part of the urinary system.
The urinary system also includes:
- two kidneys
- two tubes called ureters that lead from the kidneys into the bladder, and
- another tube called the urethra that leads out of the bladder.
In males, the urethra is a long tube that passes through the prostate and down the penis. In females, the urethra is shorter and opens in front of the vagina (birth canal).
The kidneys produce urine, which travels to the bladder through the ureters. The bladder is like a balloon and expands as it fills with urine. A layer of muscle wraps around the urethra and works like a valve to keep the bladder closed and stop leaking.
When you are ready to empty your bladder, the bladder muscle tightens and the valves open, and urine passes through the urethra and out of the body.
There are four main layers of tissue in the bladder:
- urothelium – the inner layer. It is lined with cells called urothelial cells that stop urine being absorbed into the body.
- lamina propria – a layer of tissue and blood vessels surrounding the urothelium.
- muscularis propria – the thickest layer. It consists of muscle that tightens to empty the bladder.
- perivesical tissue – the outer layer. It is mostly made up of fatty tissue, and separates the bladder from nearby organs.
Upper Tract Urothelial Cancer
Urothelial carcinoma occasionally starts in a ureter or part of a kidney. This is known as upper tract urothelial cancer.
For information about how this cancer is diagnosed and treated, see our Understanding Upper Tract Urothelial Cancer fact sheet.
Learn more
Main types of bladder cancer
There are three main types of bladder cancer, which are named after the cells they start in:
- urothelial carcinoma (80–90% of all bladder cancers) – starts in the urothelial cells lining the bladder wall. It is also called transitional cell carcinoma (TCC). Includes two rarer subtypes (plasmacytoid and micropapillary), which are more aggressive.
- squamous cell carcinoma (1–2% of all bladder cancers) – starts in thin, flat squamous cells in the bladder lining. It is more likely to be invasive.
- adenocarcinoma (about 1% of all bladder cancers) – develops from the glandular cells in the bladder. It is usually invasive.
There are also rarer types of bladder cancer. These include sarcomas, which start in the muscle, and an aggressive form called small cell carcinoma.
How common is bladder cancer?
Each year, almost 3100 Australians are diagnosed with bladder cancer. Most people diagnosed with bladder cancer are 60 or older, but it can occur at any age.
About one in every 140 males will be diagnosed with bladder cancer before age 75, making it one of the 10 most common cancers in males.
For females, the risk is about one in 560, although it is often diagnosed at an advanced stage.
Learn more
Symptoms of bladder cancer
Sometimes bladder cancer doesn’t have many symptoms and is found when a urine test is done for another reason. However, most people with bladder cancer do have some symptoms, which can include:
- Blood in the urine (haematuria) – this is the most common symptom of bladder cancer. It often happens suddenly, but is usually not painful. There may be only a small amount of blood in the urine, and it may look red or brown. The blood may come and go, or it may appear only once or twice.
- Changes in bladder habits – changes may include a burning feeling when passing urine (weeing or peeing), needing to pass urine more often or urgently, not being able to urinate when you feel the urge, and pain while urinating.
- Other symptoms – less commonly, people have pain in one side of their lower abdomen (belly) or back. They may also lose their appetite and lose weight.
Not everyone with these symptoms has bladder cancer, but if you do have any or are concerned, see your doctor as soon as possible.
If you notice any blood in your urine, see your doctor and arrange to see a specialist to have your bladder examined. The earlier bladder cancer is detected, the easier it is to treat.
Risk factors
Research shows that people with certain risk factors are more likely to develop bladder cancer. These include:
- Smoking – cigarette smokers are up to three times more likely than non-smokers to develop bladder cancer.
- Older age – about 90% of people diagnosed with bladder cancer in Australia are over 60.
- Being male – men are around three times more likely than women to develop bladder cancer.
- Chemical exposure at work – chemicals called aromatic amines, benzene products and aniline dyes are linked to bladder cancer. These chemicals are used in rubber and plastics manufacturing, in the dye industry, and sometimes in the work of painters, machinists, printers, hairdressers, firefighters and truck drivers.
- Parasitic bladder infections – squamous cell carcinoma of the bladder has been linked to a parasitic bladder infection called schistosomiasis. This is very rare in people born in Australia; it is caused by a parasite found in fresh water in Africa, Asia, South America and the Caribbean.
- Long-term catheter use – using urinary catheters over a long period may be linked with squamous cell carcinoma of the bladder.
- Previous cancer treatments – these include the chemotherapy drug cyclophosphamide and radiation therapy to the pelvic area.
- Diabetes treatment – the diabetes drug pioglitazone can increase the risk of bladder cancer.
- Personal or family history – having one or more close blood relatives diagnosed with bladder cancer, or having inherited a gene linked to bladder cancer, slightly increases the risk of bladder cancer.
Learn more about preventing cancer
Health professionals you may see
Your general practitioner (GP) will arrange the first tests to assess your symptoms. If these tests do not rule out cancer, you will usually be referred to a specialist called a urologist.
The specialist will arrange further tests. If bladder cancer is diagnosed, the urologist will consider treatment options. Often the urologist will discuss your treatment options at what is known as a multidisciplinary team (MDT) meeting.
During and after treatment, you will see a range of health professionals who specialise in different aspects of your care, including a continence nurse, stomal therapy nurse, dietician and exercise physiologist, among others.
Question checklist
Asking your doctor questions will help you make an informed choice. You may want to include some of the questions below in your own list.
Diagnosis
- What type of bladder cancer do I have?
- Has the cancer spread? If so, where has it spread? How fast is it growing?
- Are the latest tests and treatments for this cancer available in this hospital?
- Will a multidisciplinary team be involved in my care?
- Are there clinical guidelines for this type of cancer?
Treatment
- What treatment do you recommend? What is the aim of the treatment?
- If an operation is recommended, how many times have you performed it?
- Are there other treatment choices for me? If not, why not?
- If I don’t have the treatment, what should I expect?
- I’m thinking of getting a second opinion. Can you recommend anyone?
- How long will treatment take? Will I have to stay in hospital?
- Are there any out-of-pocket expenses not covered by Medicare or my private health cover? Can the cost be reduced if I can’t afford it?
- How will we know if the treatment is working?
- Are there any clinical trials or research studies I could join?
Side effects
- What are the risks and possible side effects of each treatment?
- Are there likely to be any long-term side effects?
- If I need the bladder removed, what are my options for storing urine?
- Will I have a lot of pain? What will be done about this?
- Can I work, drive and do my normal activities while having treatment?
- Will the treatment affect my sex life and fertility?
- Should I change my diet or physical activity during or after treatment?
- Are there any complementary therapies that might help me?
After treatment
- How often will I need check-ups after treatment?
- If the cancer returns, how will I know? What treatments could I have?
