Page last updated: June 2024
The information on this webpage was adapted from Understanding Prostate Cancer - A guide for people with cancer, their families and friends (2024 edition). This webpage was last updated in June 2024.
Expert content reviewers:
This information was developed based on Australian and international clinical practice guidelines, and with the help of a range of health professionals and people affected by prostate cancer:
- Prof Declan Murphy, Consultant Urologist, Director – Genitourinary Oncology, Peter MacCallum Cancer Centre and The University of Melbourne, VIC
- Alan Barlee, Consumer
- Dr Patrick Bowden, Radiation Oncologist, Epworth Hospital, Richmond, VIC
- Bob Carnaby, Consumer
- Dr Megan Crumbaker, Medical Oncologist, St Vincent’s Hospital Sydney, NSW
- Henry McGregor, Health Physiotherapist, Adelaide Men’s Health Physio, SA
- Jessica Medd, Senior Clinical Psychologist, Department of Urology, Concord Repatriation General Hospital and Headway Health, NSW
- Dr Gary Morrison, Shine a Light (LGBTQIA+ Cancer Support Group)
- Caitriona Nienaber, 13 11 20 Consultant, Cancer Council WA;
- Graham Rees, Consumer
- Kerry Santoro, Prostate Cancer Specialist Nurse Consultant, Southern Adelaide Local Health Network, SA
- Prof Phillip Stricker, Chairman, Department of Urology, St Vincent’s Private Hospital, NSW
- Dr Sylvia van Dyk, Brachytherapy Lead, Peter MacCallum Cancer Centre, VIC.
Prostate cancer begins when abnormal cells in the prostate start growing in an uncontrolled way.
The prostate
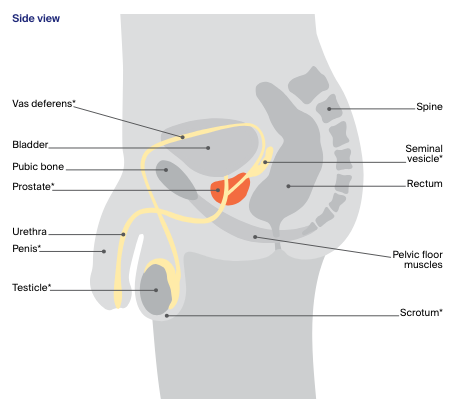
The prostate is a small gland about the size of a walnut. It forms part of the male reproductive system.
The prostate sits below the bladder and in front of the rectum (the end section of the large bowel). Two glands called the seminal vesicles attach to the back of the prostate.
The prostate is close to nerves, blood vessels, and muscles that help control erections and urination (the pelvic floor muscles and urinary sphincter).
What the prostate does
The prostate produces fluid that helps to feed and protect sperm. This fluid forms part of semen. Semen also contains sperm made in the testicles (testes) and fluid made by the seminal vesicles.
- Urethra – this is a thin tube that runs from the bladder and through the prostate to take urine (wee or pee) out of the body. The urethra also carries semen during orgasm.
- Ejaculation – when an orgasm occurs, millions of sperm from the testicles move through two tubes near the prostate called the vas deferens. The sperm then join with the fluids produced by the prostate and seminal vesicles to make semen. The muscle around the prostate contracts and pushes the semen into the urethra and out through the penis.
How the prostate grows
The male sex hormone, testosterone, is made by the testicles and controls how the prostate grows. It is normal for the prostate to become larger with age. This may lead to a condition known as benign prostate hyperplasia (BPH).
How common is prostate cancer?
Prostate cancer is the most common cancer in Australian men (except for skin cancer). About 1 in 12 men will get prostate cancer by the age of 70, and 1 in 5 will get it in their lifetime.
About 25,500 men are diagnosed each year, and rates are increasing. This may be in part because the population is growing and people may be living longer.
Anyone with a prostate can get prostate cancer – men, transgender women and intersex people. See our LGBTQI+ communities page for more information. For information specific to you, speak to your doctor.
More prostate cancer statistics and trends
Risk factors
Factors that increase the risk of developing prostate cancer include:
- getting older – especially being aged 50 and over1 (more than 90% of people diagnosed with prostate cancer are aged 55 and over)
- family history of prostate, breast or ovarian cancer
- being of African or African-American descent.
While prostate cancer is less common if you are aged 50 and under, people aged 40 and over may have a higher than average risk of developing prostate cancer later in life if their prostate specific antigen (PSA) test results are higher than the typical range for their age.
What screening test should I have?
Cancer screening is testing to look for cancer in people who don’t have any symptoms. The benefit of screening is that the cancer can be found and treated early.
However, it is important that the benefits of screening outweigh any potential harms from treatment side effects. There is currently no national screening program for prostate cancer (national guidelines were under review as of May 2024).
The prostate specific antigen (PSA) blood test may identify fast-growing cancers that can spread to other parts of the body and would benefit from treatment.
It may also find slow-growing cancers unlikely to be harmful, for which having treatment may cause significant side effects.
Some people without symptoms of prostate cancer choose to have regular PSA tests. It is important to talk to your doctor about the benefits and risks in your particular circumstances before having a PSA.
If you choose to have regular PSA tests, the current guidelines recommend that:
- men with no family history of prostate cancer have PSA testing every 2 years from age 50–69
- men with a family history of prostate cancer have PSA testing every 2 years starting from age 40–45 (depending on how strong the family history is) to age 69.
At-home PSA test kits are not recommended. The tests could be unreliable and do not come with qualified medical advice about the results. A PSA screening test, requested by your doctor, should be available to you for free.
Your doctor will also be able to explain what the results of your test mean, and can also refer you for other tests you may need.
Learn more about prostate testing
Complementary or herbal supplements claiming to reduce PSA readings, or to prevent PSA from rising, are not recommended by Cancer Council. They may mask your true PSA, or cause you to have false results on medical pathology PSA testing.
Does prostate cancer run in families?
Having a strong family history of cancer may increase the risk of developing prostate cancer. You may have inherited a gene that increases your risk of prostate cancer if you have:
- several close relatives on the same side of the family (either your mother’s or father’s side) diagnosed with prostate, breast and/or ovarian cancer, especially if due to a fault in the BRCA1 or BRCA2 genes
- a brother or father diagnosed with prostate cancer before age 60. In this case your risk is twice that of others.
If you are worried about your family history, talk to your GP. They may refer you to a family cancer clinic or genetic counselling service. For more information, call 13 11 20 cancer support.
More about genetics and risk
Symptoms
Early prostate cancer rarely causes symptoms. Even people diagnosed with advanced prostate cancer may have no symptoms.
Difficulty passing urine is not always a symptom of prostate cancer, but you should see your doctor if you are worried or the following symptoms are ongoing:
- frequent or sudden need to urinate
- blood in the urine or semen
- a slow flow of urine
- needing to get up at night to pass urine
- feeling like your bladder is not empty after passing urine
- unexplained weight loss
- pain in bones, for example the neck, back, hips or pelvis.
Non-cancerous changes to the prostate
A normal prostate often grows larger as you age and is called benign prostate hyperplasia (BPH). It is not usually due to cancer but BPH may press on the urethra and affect how you urinate (pee). You may:
- notice a weak stream of urine
- go to the toilet more often, especially at night
- need to pee urgently
- have trouble starting to pee
- dribble urine after peeing
- feel that the bladder is not empty.
Talk to your doctor if you have any of these urinary symptoms – because they can also happen in advanced prostate cancer.
Find a Health Professional
Health professionals you will see
Your GP will arrange the first tests to assess your symptoms. If these tests do not rule out cancer, you will usually be referred to a specialist, who will arrange further tests.
Prostate cancer is usually diagnosed by a urologist, who will talk to you about your surgical or other options.
You will usually also see a radiation oncologist to discuss radiation therapy. You may be referred to a medical oncologist who will discuss drug treatments.
It's important to find out all your options before making a decision. Your specialists will discuss treatment options with other health professionals at what is known as a multidisciplinary team (MDT) meeting.
During and after treatment, you will see a range of health professionals who specialise in different aspects of your care, including an endocrinologist, continence nurse, pathologist and sexual health physician, among others.
Question checklist
Asking your doctor questions will help you make an informed choice. You may want to include some of these questions in your own list:
Diagnosis
- What type of prostate cancer do I have?
- Has the cancer spread? If so, where has it spread? What is the grade?
- Are the latest tests and treatments for this cancer available in this hospital?
- Will a multidisciplinary team be involved in my care?
- Are there clinical guidelines for this type of cancer?
Treatment
- What treatment do you recommend? What is the aim of the treatment?
- Have you treated a lot of people with my type of cancer?
- Are there other treatment choices for me? If not, why not?
- If I don’t have the treatment, what should I expect?
- How long do I have to make a decision?
- I’m thinking of getting a second opinion. Can you recommend anyone?
- How long will treatment take? Will I have to stay in hospital?
- Are there any out-of-pocket expenses not covered by Medicare or my private health cover? Can the cost be reduced if I can’t afford it? Can I be treated in the public system?
- How will we know if the treatment is working?
- Are there any clinical trials or research studies I could join?
Side effects and follow-up
- What are the risks and possible side effects of each treatment? How can these be managed?
- If I have problems with continence, what can I do to manage this?
- Will the treatment affect my sex life and erections? What can be done about this? Which health professionals should I see?
- Will I still be able to have children? Should I see a fertility specialist?
- Are there any complementary therapies that might help me?
- How often will I need check-ups after treatment?
- If the cancer returns, how will I know? What treatments could I have?
Your guide to best cancer care
A lot can happen in a hurry when you’re diagnosed with cancer. The guide to best cancer care for prostate cancer can help you make sense of what should happen.
It will help you with what questions to ask your health professionals to make sure you receive the best care at every step.
Read the guide
