What is ocular melanoma?
There are many different types of cancer that can affect the eye, but ocular melanoma is the most common. Melanoma is a type of cancer that develops in cells that produce melanin — the pigment that gives skin its colour. Your eyes also have melanin-producing cells and can develop melanoma.
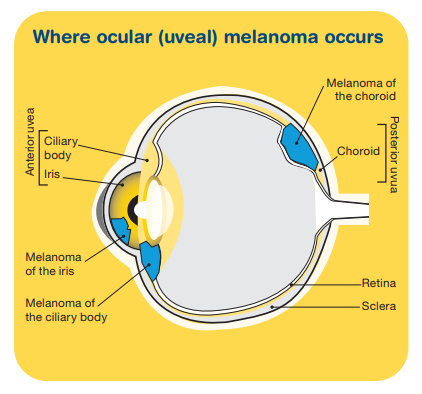
Ocular melanoma is also known as uveal melanoma. The uvea is the middle layer of the eye beneath the white part and consists of the iris, ciliary body and choroid. Melanoma can occur in any of these parts. It can also be named according to the part of the eye it started in.
- The iris – the coloured part of the eye which helps regulate the amount of light entering the eye.
- The ciliary body – the part of the eye that controls the shape of the lens and makes the fluid in the eye, which provides nutrition and maintains pressure.
- The choroid or posterior uvea – the vascular layer of the eye between the retina and the white outer layer (sclera). Ocular melanoma more commonly develops here.
Ocular melanoma is much rarer than skin melanoma and behaves very differently. Melanomas that develop on the skin usually occur on parts of the body that have been exposed to the sun. Some melanomas, however, can also start inside the eye or in a part of the body that has never been exposed to the sun.
Most ocular melanomas develop in the part of the eye that you can’t see when looking in a mirror, which makes it hard to diagnose.
The eye
The human eye is a sense organ that reacts to light and allows us to see. Your eye works in a similar way to a camera. When you look at an object, light passes through the cornea (the clear front layer of the eye) and enters the eyes through the pupil (the black centre of the eye). The iris (the coloured part of the eye) controls how much light the pupil lets in.
Light then passes through the lens (the clear inner part of the eye) which, together with the cornea, focuses light onto the retina. When light hits the retina (layer of tissue at the back of the eye) special cells called photoreceptors convert the light into electrical impulses that travel through the optic nerve to the brain. The brain then turns these signals into the images that you see.

How common is ocular melanoma?
Ocular (uveal) melanoma is rare. Each year, around 125–150 Australians are diagnosed with this type of cancer (about 5–6 cases per million people). It is more likely to be diagnosed in men than women, and can occur at any age, but the risk increases with age.
Learn more about rare cancer
Risk factors
The cause of ocular melanoma is not known in most cases. However, there are several risk factors:
- having pale or fair skin – people whose skin burns easily are most at risk.
- having a light eye colour – people with blue or green eyes have a greater risk than people with darker eyes.
- family history of melanoma – a very small number of people who have melanoma have inherited a faulty gene.
- having a growth on or in the eye – people with an 'eye freckle' may be at risk.
- age – the risk increases with age.
- certain skin conditions and pigmentation – some people have a skin disorder (dysplastic naevus syndrome) which causes moles to grow abnormally, and this can increase your risk.
- occupational exposure – being exposed to UV radiation or certain chemicals at work, particularly through welding, can increase your risk.
Symptoms
Ocular melanoma can be difficult to diagnose as it forms in the part of the eye that isn’t visible to you or others. It doesn’t typically cause any signs and symptoms and is usually detected by an optometrist during a routine eye test. Symptoms that some people may experience include:
- poor or blurred vision in one eye
- loss of peripheral vision
- brown or dark patches on the white of the eye
- a dark spot on the iris
- small specks, wavy lines or ‘floaters’ in your vision
- flashes in your vision
- a change in the shape of the pupil.
These symptoms can be caused by other eye conditions, but if you experience any, you need to discuss them with your doctor.
Diagnosis
If your doctor or optometrist thinks that you may have ocular melanoma, they will carry out certain tests. If the results suggest that you may have ocular melanoma, your doctor will refer you to a specialist doctor called an ophthalmologist who treats eye disorders.
Further tests
The ophthalmologist will carry out more tests that may include:
- Ophthalmoscopy (funduscopy) – a test that allows your doctor to look at the inside of your eye to check for abnormalities. You may be asked to look into a large microscope, so the doctor may not have to perform a biopsy to determine if a tumour is present.
- Colour fundus photography – photographs of the back of your eye will be taken and can help show what the tumour looks like before and after treatment.
- Ultrasound scan – this painless test uses soundwaves to create pictures of the inside of your eye and surrounding areas. For this scan a gel will be spread over your closed eyelid and a small device called a transducer is moved over the area to accurately show the size of the tumour.
- Transillumination – if you need surgery, this test may be done first to show exactly where the melanoma is. The lights in the room are turned down and the doctor shines a very bright light into your eye to look for abnormal areas.
- CT or MRI scans – special painless machines are used to scan and create pictures of the inside of your body to find tumours or check for any spread of disease. Before the scan you may have an injection of dye into one of your veins, which makes the pictures clearer.
- Biopsy – most of the time, the ophthalmologist can make a diagnosis from what they see when they examine your eye, from photographs and ultrasound pictures. However, sometimes a biopsy is performed. In a biopsy, some tissue is removed from the affected area so it can be examined more closely under a microscope.
Treatment
Discussion with your doctor will help you decide on the best treatment for your cancer depending on:
- the site of the cancer you have (choroid, ciliary body or iris)
- size of the cancer
- how close the cancer is to other parts of the eye
- whether or not the cancer has spread
- your age, fitness and general health
- your preferences.
The main factors in deciding what treatment you will have are the location and size of the tumour and wanting to save the sight of your eye. Preserving how your eye looks is also important.
You will be treated by a multi-disciplinary team (MDT) of health professionals who specialise in different areas of your care. The team may include a radiation oncologist, medical oncologist, occupational therapist and counsellor, among others.
Surgery
Surgery for ocular melanoma can include:
- Iridectomy – removal of part of the iris (coloured part of the eye).
- Iridocyclectomy – removal of part of the iris and the ciliary body.
- Endoresection or transscleral resection – removal of only the tumour in the ciliary body or choroid.
- Enucleation – removal of the entire eye. This is performed for larger melanomas or if the vision in the eye has already been lost. An artificial eye matching your eye size and colour will usually be inserted after surgery to replace the eye.
- Orbital exenteration – removal of the eye and some surrounding tissue.
These operations are done while you are under a general anaesthetic and you will have to stay in hospital for one or two days. Common side effects can include loss of vision, damage to nearby tissue, pain, bleeding, blood clots and an increased risk of infection.
Radiation therapy
Radiation therapy uses high energy rays to destroy cancer cells. It may be used for ocular melanoma:
- after surgery, to destroy any remaining cancer cells and stop the cancer coming back
- if the cancer can’t be removed with surgery
- instead of removing the eye
- if the cancer has spread to other parts of the body (e.g. palliative radiation to control symptoms).
For ocular melanoma, radiation therapy is given the following ways:
Plaque radiation therapy (plaque brachytherapy) – small seeds of radioactive material are placed in a small disc (called a plaque) and attached to the wall of the eye over the tumour during an operation. Radiation is then delivered to the tumour. The plaque is left in place until the right amount of radiation has been given. This is usually about four to five days and you will have to stay in hospital during this time. After this, you will have another short operation to remove the plaque.
Proton beam radiation therapy – proton beams are aimed directly at the tumour and may cause less damage to the other tissues they pass through. Treatment is given in high doses over several days. This treatment is currently not available in Australia but check with your radiation oncologist.
Stereotactic radiation therapy – multiple small beams of radiation are used to precisely target the tumour in high doses. You usually need five sessions given over ten days. A course of stereotactic radiation therapy needs to be carefully planned.
Radiation therapy does not hurt and is usually given over a period of time to minimise side effects, which commonly include blurry vision, dry eye, cataracts, glaucoma, loss of vision, eye discomfort and
fatigue.
Other treatments
Laser treatment (transpupillary thermotherapy) or photodynamic therapy – this treatment uses an infrared laser to heat and destroy cancer cells. It is sometimes combined with photodynamic therapy which uses a laser combined with a light-sensitive drug to destroy cancer cells. The drug is injected into your vein and makes the cells in your body more sensitive to light. The treatment is painless, but you will be sensitive to light for several days after treatment. Common side effects can include loss of vision, eye discomfort and bleeding inside the eye.
Immunotherapy – if the ocular melanoma has spread to other parts of the body, immunotherapy may be considered. This treatment has been very helpful in treating metastatic skin melanoma and uses drugs to stimulate your own immune system to recognise and attack cancer cells. Common side effects can include infection, fatigue, skin reactions, headaches, kidney problems and inflammation of the heart, colon and liver.
Clinical trials – your doctor may suggest you take part in a clinical trial. Doctors run clinical trials to test new or modified treatments and ways of diagnosing disease to see if they are better than current methods. Over the years, trials have improved treatments and led to better outcomes for people with cancer.
Complementary therapies – complementary therapies are designed to be used alongside conventional medical treatments (such as surgery and radiation therapy) and can increase your sense of control, decrease stress and anxiety, and improve your mood.
Question checklist
Asking your doctor questions will help you make an informed choice. You may want to include some of the questions below in your list.
- What type of ocular melanoma do I have?
- Has the cancer spread? What stage of cancer do I have?
- Will I lose my eyesight?
- What are the treatment options for me? What do you recommend and why?
- What are the possible risks and side effects of my treatment? How will these be managed?
- Have you treated this type of cancer before?
- How complex is the surgery and how long does the operation take?
- How long will treatment take?
- Is this treatment covered by Medicare/private insurance? Will there be extra expenses?
- Are there any complementary therapies that might help me?
- If the cancer comes back, how will I know?
- What are the possible benefits and risks to joining a clinical trial? What is being tested and why? How many people will be involved in this research?
Life after treatment
Once your treatment has finished, you will have regular check-ups to confirm the cancer hasn’t come back. Ongoing surveillance for ocular melanoma involves a schedule of tests and scans, eye tests and physical examinations.
For some people ocular melanoma does come back after treatment, which is known as a recurrence. If the cancer does come back, treatment will depend on where the cancer has returned in your body and may include a mix of surgery, radiation therapy, laser and immunotherapy.
In some cases of advanced cancer, treatment will focus on managing any symptoms, such as pain, and improving your quality of life without trying to cure the disease. This is called palliative treatment and it can be provided in the home, hospital, palliative care unit or hospice, or residential aged care facility.
Learn more
Understanding Ocular (Uveal) Melanoma
Download our Understanding Ocular (Uveal) Melanoma fact sheet to learn more
Download now
Expert content reviewers:
A/Prof William Glasson, Ophthalmologist, Queensland Ocular Oncology Service, Queensland; Dr Lindsay McGrath, Ophthalmic Surgeon, Queensland Ocular Oncology Service, Queensland; Caitriona Nienaber, 13 11 20 Consultant, Cancer Council WA; Jane Palmer, Senior Oncology Nurse and Researcher, Oncogenomics Laboratory, QIMR Berghofer Medical Research Institute, Queensland Ocular Oncology Service, Queensland; Katrina Potter, Consumer; Susan Vine, OcuMel Australia; Ann Marie Weber, Consumer; Dr Wenchang Wong, Senior Radiation Oncologist, Prince of Wales Hospital, Sydney, Conjoint Senior Lecturer, University of NSW.
Page last updated:
The information on this webpage was adapted from Understanding Ocular (Uveal) Melanoma - A guide for people affected by eye cancer (2021 edition). This webpage was last updated in August 2021.
