Page last updated: April 2025
The information on this webpage was adapted from Understanding Neuroendocrine Tumours (NETs) - A guide for people with cancer, their families and friends (2025 edition). This webpage was last updated in April 2025.
Expert content reviewers:
This information is based on clinical practice guidelines and has been developed with help from health professionals and people affected by neuroendocrine tumours. It was reviewed by:
- Prof Michael Michael, Gastrointestinal and Neuroendocrine Medical Oncologist and Co-Chair Neuroendocrine Unit, Peter MacCallum Cancer Centre, VIC
- Tracey Bilson, Consumer
- Meredith Cummins and Kahlia Wolsley, NeuroEndocrine Cancer Australia
- Dr Ganessan Kichenadasse, Medical Oncologist and Pharmacologist, Flinders Medical Centre, SA
- Dr Nat Lenzo, Nuclear Medicine Physician, ICON, WA
- A/Prof David Pattison, Co-Director, Department of Nuclear Medicine & PET Services, Royal Brisbane & Women’s Hospital, QLD
- Prof Jas Samra, Head of Upper GI Surgery, RNSH and Clinical Prof of Surgery, University of Sydney, NSW
- Jillian van Zijl, 131120 Consultant, Cancer Council WA
- A/Prof David Wyld, Director, Medical Oncology, Royal Brisbane & Women’s Hospital, QLD
What are NETs?
The neuroendocrine system is made up of many glands and nerve cells all over the body that produce hormones and then release them into the bloodstream. These hormones help control how the body works, for example, in digesting food.
NETs, also called neuroendocrine neoplasms (NENs), are a rare group of tumours that develop from neuroendocrine cells that become abnormal and keep growing.
All NETs are considered cancer (malignant), but some grow slowly (low grade) while some grow quickly (high grade). The high grade tumours are also known as neuroendocrine carcinomas (NECs).
Malignant tumours can spread through the bloodstream or lymph vessels and form another tumour at other parts of the body. This new tumour is known as secondary cancer or metastasis.
Types of NETs
NETs are grouped according to where in the body the cancer started. Some NETs make extra hormones, which can cause certain symptoms. These are referred to as functional tumours.
NETs that do not produce extra hormones are known as non-functional tumours.
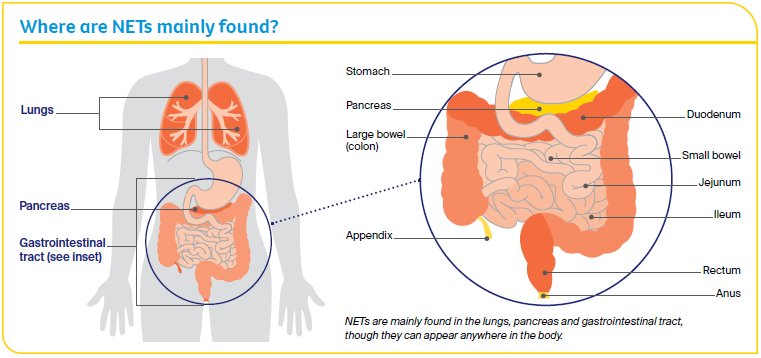
Gastrointestinal
These NETs start in the gastrointestinal (GI) tract, which is part of the digestive system. They include:
- gastric NETs, in the stomach
- duodenal NETs
- small bowel NETs, including the jejunum and ileum
- large bowel NETs, in the colon
- appendiceal NETs
- rectal NETs, near the anus.
Pancreatic
The pancreas is a long, flat gland that lies between your stomach and spine. It makes digestive juices and hormones. Pancreatic NETs start in the neuroendocrine cells of the pancreas and make up about 5% of cancers in the pancreas.
Most (about 90%) of pancreatic NETs do not produce extra hormones and are called non-functioning. Functional pancreatic NETs are rare and most are named after the hormone they overproduce:
- insulinomas produce too much insulin
- glucagonomas produce too much glucagon
- gastrinomas produce too much gastrin
- somatostatinomas produce too much somatostatin
- VIPomas produce too much of a substance called vasoactive intestinal peptide.
Lung
Lung NETs make up about 14% of lung cancers. The 4 subtypes of lung NETs are:
- typical carcinoids
- atypical carcinoids
- large cell neuroendocrine carcinomas
- small cell lung neuroendocrine cancer.
Other NETs
Merkel cell carcinoma is a fast-growing cancer in cells in the top layer of the skin. For a directory of specialists in Merkel cell carcinoma care and treatment, visit the Australian Merkel Cell Carcinoma Interest Group.
Neuroblastoma, a tumour in the adrenal glands above the kidneys, is more commonly diagnosed in children. For more information, contact Neuroblastoma Australia.
For more information on other types of NETs, including thymic, testicular, prostate, ovarian and endometrial, multiple endocrine neoplasia (MEN), pheochromocytoma, paraganglioma and medullary thyroid carcinoma, visit NeuroEndocrine Cancer Australia.
How common are NETs?
NETs are not common but the number of people being diagnosed is slowly increasing. There is an almost equal risk for males and females.
Around 5700 Australians are diagnosed with a specific NET each year, with most new cases being diagnosed in people aged 40 years or over (according to the Australian Institute of Health and Welfare).
Learn more about rare cancer
Risk factors
The causes of most NETs are not known. However, some factors increase the risk of developing certain types of NETs. Having these risk factors does not mean you will develop a NET, but if you are concerned, talk to your doctor.
People with some rare, inherited diseases have a higher risk of NETs. These include multiple endocrine neoplasia (MEN 1, MEN 2), Von Hippel- Lindau (VHL) syndrome, tuberous sclerosis complex (TSC) and neurofibromatosis (NF).
Some NETs are more likely in certain people, such as those who have:
- conditions that affect stomach acid, such as pernicious anaemia, peptic ulcers and chronic atrophic gastritis
- inflammatory bowel disease
- diabetes – which may increase the risk of pancreatic NETs
- exposure to cancer-causing substances
- certain gene mutations, such as succinate dehydrogenase subunit genes (SDHx), which can increase the risk of tumours, paragangliomas and phaeos in the kidneys and GI tract.
Specific NETs can occur in certain age groups, such as appendiceal NETs in younger people, neuroblastoma in children under 5, or Merkel cell carcinoma in older men.
Your guide to best cancer care
A lot can happen in a hurry when you’re diagnosed with cancer. The guide to best cancer care for neuroendocrine tumours can help you make sense of what should happen.
It will help you with what questions to ask your health professionals to make sure you receive the best care at every step.
Read the guide
Symptoms
Most NETs develop slowly over several years but they can also be aggressive and grow quickly, spreading to other parts of the body and causing problems.
In the early stages, NETs may not cause symptoms. If you do have symptoms, they will depend on where in the body the tumour is and if the tumour cells are making hormones. It is common to feel tired or lose your appetite.
Gastrointestinal
Symptoms may include:
- abdominal (tummy) pain and bloating
- changes in bowel or bladder habits, including diarrhoea
- bowel obstruction (blockage) or bleeding from the anus
- redness of the face or neck, and rashes
- wheezing
- fast heartbeat.
Lung
Symptoms may include:
- repeated pneumonia or chest infections
- coughing up blood
- shortness of breath
- wheezing
- chest pain.
Pancreatic
Non-functional pancreatic NETs – These do not produce extra hormones and rarely cause symptoms in the early stages. Symptoms usually appear when the tumour is large enough to affect nearby organs, or spreads (most commonly to the liver). As the tumour grows, it may also cause weight loss and pain in the upper abdomen, side or back.
Functional pancreatic NETs – These produce too many hormones, which can sometimes cause the first symptoms.
Symptoms may include:
- low blood sugar levels (hypoglycaemia), causing shaking, sweating, confusion, dizziness and fast heartbeat
- high blood sugar levels (hyperglycaemia), causing increased urination (weeing), excessive thirst and blurry vision
- indigestion (heartburn) and stomach ulcers
- rash in the groin or armpit area
- losing weight for no reason
- nausea or vomiting
- changes in bowel habits, including diarrhoea or pale, foul-smelling stools that are hard to flush.
Carcinoid syndrome
When NETs make a large amount of hormones (such as serotonin), this can cause a group of symptoms known as carcinoid syndrome. These symptoms may include:
- redness of the face or neck
- diarrhoea
- wheezing
- fast heartbeat
- carcinoid heart disease.
Carcinoid syndrome is most common in people with gastrointestinal NETs, including duodenal and small bowel, and lung NETs that have spread (metastasised). However, not everyone with these NETs will develop carcinoid syndrome.
More information is available from NeuroEndocrine Cancer Australia.
When the cancer is advanced
Because NETs are relatively difficult to diagnose and symptoms may be confused with other health conditions, a NET may be advanced when found, it may spread, or it may come back after treatment.
If this happens, there may still be treatments to remove the cancer or help control its growth and manage symptoms.
Advanced NETs may not be cured, but they can be controlled with treatment, sometimes for a very long time.
Treatment will depend on the type of NET, how far it has spread, your general health, treatment goals or preferences, and quality of life.
Learn more
Diagnosis
NETs can be difficult to diagnose and are sometimes found when doctors are testing for a different condition.
If your doctor thinks that you may have a NET (or one of the syndromes associated with NETs), they will ask about your medical history, do a physical examination and run some tests.
If the results suggest that you may have a NET, your doctor will refer you to a specialist, who will usually carry out one or more of the tests listed below.
Tests and scans
- Blood tests – a full blood count to measure your white blood cells, red blood cells and platelets and a hormone marker called chromogranin A.
- Urine tests – these measure the hormone serotonin (which can be produced by NETs).
- Endoscopy – a thin, flexible tube with a light and camera (endoscope) is inserted down the throat to examine the digestive tract.
- Gastroscopy – an examination of the large bowel with a camera on a flexible tube (colonoscope) which is passed through the anus.
- Bronchoscopy – a flexible tube with a light and camera is inserted down the throat to examine the airways and lungs and take tissue samples.
- imaging scans – CT (computerised tomography), PET (positron emission tomography) and MRI (magnetic resonance imaging) scans use special machines to create pictures of the inside of your body while you lie still on an examination table. Before the scan, you may have an injection of dye (called contrast) or glucose into one of your veins, which makes the pictures clearer. The 2 different types of PET scans used for NETs are Gallium-68 Dotatate (also called Gatate scans) and fluorodeoxyglucose (FDG). The scan you have will depend on the type and grade of tumour.
- Biopsy – this removes a sample of tissue from the affected area for examination under a microscope. It is done either with a thin needle inserted into the tumour under local anaesthetic, or under general anaesthesia, known as an open biopsy.
- Echocardiogram – an ultrasound scan of the heart to check how it is working.
For a directory of specialists in NET care and treatment, contact NeuroEndocrine Cancer Australia.
Question checklist
If you have a NET, asking your doctor questions will help you make an informed choice. You may want to make a list of questions before appointments and include some of these questions:
- What type of NET do I have? Where is it located?
- How far has it spread? What stage of cancer do I have?
- What grade is my tumour/tumours?
- Have you treated this type of cancer before?
- What are the treatment options for me? What do you recommend and why?
- What is the goal of treatment for my type of NET?
- What are the possible risks and side effects of my treatment? How will these be managed?
- What impact will treatment have on my fertility?
- How long will treatment take?
- Is this treatment covered by Medicare/private insurance? Will there be extra expenses?
- If the cancer comes back, how will I know?
If you are thinking of taking part in a clinical trial, here are some questions you could ask:
- What are the possible benefits and risks to me?
- What is being tested and why?
- How many people will be involved in this trial?
- If I cannot get onto a clinical trial, can I still pay for a drug that is currently in a trial?
“I kept a notebook to record my symptoms and any questions I had for my oncologist.” Meg
Treatment
The treatment you have for NETs depends on:
- the tumour type
- its size
- how fast it is growing and where it is in your body
- your age, fitness and overall health, and
- any symptoms you may have.
Your treatment team may include a surgeon, medical oncologist, radiation oncologist, nuclear medicine specialist, gastroenterologist, interventional radiologist, endocrinologist, nurses and allied health professionals such as a dietitian, social worker, physiotherapist and occupational therapist.
The aim of treatment is to remove the cancer (curative), or to manage symptoms and improve quality of life.
It can feel overwhelming to decide on treatment. If the cancer was diagnosed at a later stage, your options may feel limited compared with a common cancer.
While some people want detailed information, others prefer to leave decisions to their doctors.
Surgery
The aim of surgery for early-stage NETs is to cure the cancer. If the cancer has spread, removing part of the tumour will help reduce symptoms and the risk of bowel obstruction in small bowel NETs.
Surgery usually involves removing the tumour and some healthy tissue around it to ensure the tumour is completely removed. The type of operation depends on the size of the tumour and where it is.
Surgery for pancreatic NETs is the same as for other types of pancreatic cancer. See the Treatment chapter in the Understanding Pancreatic Cancer booklet for more information.
Side effects of NET surgery may include changes to bowel movements, pain and discomfort, fatigue, a higher risk of infection, scarring, and temporary or permanent damage to nearby organs.
Talk to your treatment team about how these can be managed.
Radiation therapy
Also known as radiotherapy, radiation therapy uses a controlled dose of radiation to kill or damage cancer cells.
In external beam radiation therapy (EBRT), the radiation comes from a large machine. You will lie on a treatment table underneath the machine, and you will not see or feel the radiation.
Radiation therapy can shrink the cancer. This may help to relieve the symptoms such as pain.
Radionuclide therapy
A type of radiation therapy called peptide receptor radionuclide therapy (PRRT) may be used for people with NETs whose tumours have a positive somatostatin receptor.
PRRT involves injecting a protein (peptide) mixed with a small amount of radioactive substance (radionuclide). This targets cancer cells and delivers a high dose of radiation to kill or damage them.
You may have a dose of chemotherapy in tablet form before PRRT as a combined treatment. The most common form of PRRT is 177Lu-Dota-octreotate (LuTate) therapy.
PRRT is available only at specialised treatment centres in each state, usually in major cities. It may also be available through clinical trials.
Drug therapies
Also known as systemic therapy, the most common forms of drug therapies for NETs are:
- Somatostatin analogues (SSAs) – Somatostatin is a hormone produced by the body. SSAs are medicines that act like this hormone and help slow down or prevent tumour growth. They are usually given as monthly injections.
- Targeted therapy – These drugs attack specific molecules within cells and work by blocking cell growth. They are given in capsules that you swallow. People with advanced pancreatic NETs may be offered targeted therapy drugs such as sunitinib and everolimus. Everolimus may also be used to treat advanced GI and lung NETs.
- Chemotherapy – Chemotherapy uses drugs to kill or slow the growth of cancer cells. People with pancreatic, bronchial or high-grade NETs may have one chemotherapy drug, or a combination of drugs and other treatments such as surgery. Chemotherapy is given through a drip into a vein (intravenously) or as a tablet that is swallowed (oral chemotherapy).
Treatment for NETs in the liver
NETs, particularly types that affect the GI system and the pancreas, often spread to the liver. These tumours are called metastases. Radionuclide therapy or chemotherapy will also treat tumours in the liver.
The choice of treatment depends on a number of factors, including where the tumours have spread. Other treatments to control NETs in the liver may include:
Radiofrequency ablation (RFA) and microwave ablation
Guided by an ultrasound or CT scan, a needle is inserted through the abdomen into the liver tumour. The needle sends out radio waves or microwaves that produce heat and destroy the cancer cells.
Transarterial chemoembolisation (TACE)
In this procedure, a catheter is inserted into the hepatic artery, which supplies blood to the liver. A chemotherapy drug together with tiny particles (called microspheres) are released into the artery, which blocks the flow of blood into the tumour.
This may cause the tumour to shrink. TACE is performed by an interventional radiologist. Sometimes the injection uses microspheres alone. This is called transarterial embolisation (TAE) or hepatic artery embolisation (HAE).
Selective internal radiation therapy (SIRT)
Also known as radioembolisation, SIRT is done by an interventional radiologist. The radiologist inserts a catheter into the main artery of the liver and then delivers tiny radioactive beads to the liver through the catheter.
The beads give a direct dose of radiation to the tumour.
Clinical trials
Your doctor or nurse may suggest you take part in a clinical trial. Clinical trials test new or modified treatments and ways of diagnosing disease to see if they are better than current methods.
For example, if you join a trial, you will be chosen at random to receive either the best existing treatment or the modified new treatment.
Over the years, trials have improved treatments and led to better outcomes for people diagnosed with cancer.
You may find it helpful to talk to your specialist or GP, or to get a second opinion. If you decide to take part in a clinical trial, you can withdraw at any time.
Learn more
Side effects of treatment
All treatments can have side effects. The type of side effects that you may have will depend on the type of treatment and where in your body the NET is. Some people have very few side effects and others have more.
Before treatment begins, your specialist team will discuss all possible side effects, both short term and long term. They may also discuss any late effects, which may not start immediately.
Common side effects of treatment for NETs include fatigue, loss of appetite, nausea, bowel and bladder changes, damage to organs near the area being treated, and lymphoedema (swelling).
Certain treatments have their own specific side effects, such as an increased chance of hair loss, blood clots or gallstones.
Effects on fertility
Some treatment for NETs can affect your ability to have children ( fertility), which may be temporary or permanent.
If it is important to you that you are able to have children in the future, talk to your doctor about what options are available.
Ways to look after yourself
Cancer can cause physical and emotional strain, so it is important to look after your wellbeing. Cancer Council has free information and programs to help you during and after treatment.
- Take a break – Make time each day just for relaxation and enjoyment. Think about things that help you to relax and feel good, such as reading, listening to music, taking a bath or having a massage. Keeping in touch with the world through work, hobbies, or time with family and friends may help you connect with your life outside of cancer and provide a break from your worries.
- Eat and drink well – Some people with NETs, especially pancreatic NETs, or those who have had bowel surgery, may need to change what they eat. Certain foods and drinks can trigger symptoms of carcinoid syndrome (facial flushing, diarrhoea), and some vitamin deficiency syndromes may be more common. You can talk to a dietitian about what to eat. NeuroEndocrine Cancer Australia has a NET specialist dietitian available and a Nutrition and Neuroendocrine Tumours booklet available.
- Be active – Research shows exercise can benefit people during and after cancer treatment. Being active can help you cope with some of the common side effects of cancer treatment and speed up recovery. It can also improve quality of life by giving you more energy, keeping your muscles strong, helping you maintain a healthy weight and boosting your mood.
- Try complementary therapies – Therapies such as massage, relaxation and acupuncture are used alongside conventional medical treatments and can increase your sense of control, decrease stress and anxiety, manage pain and improve your mood. Let your doctor know about any therapies you are thinking of trying, as some may not be safe or evidence-based.
- Sort out issues – A cancer diagnosis can cause or add to financial problems, work-related issues, accommodation difficulties, relationship concerns and family stresses. There is support available – talk to the hospital social worker or call Cancer Council 13 11 20.
- Develop a care plan – Some cancer centres help you develop a “survivorship care plan”. This plan includes a summary of treatment, a schedule for follow-up care, symptoms to watch out for and possible long-term side effects, potential medical or emotional issues and suggestions on living a healthy lifestyle. See NeuroEndocrine Australia's Treatment and Wellness Care Plan for a template to record your ongoing care.
Understanding Neuroendocrine Tumours (NETs)
Download our Understanding NETs fact sheet to learn more
Download now
