Page last updated: June 2024
The information on this webpage was adapted from Understanding Brain Tumours - A guide for people with cancer, their families and friends (2024 edition). This webpage was last updated in June 2024.
Expert content reviewers:
This information was developed based on Australian and international clinical practice guidelines, and with the help of a range of health professionals and people affected by brain tumours:
- Prof Lindy Jeffree, Director of Neurosurgery, Alfred Health, VIC
- Caitriona Nienaber, 13 11 20 Consultant, Cancer Council WA
- Prof Tamara Ownsworth, Clinical Neuropsychologist and Research Director, The Hopkins Centre, Griffith University, QLD
- A/Prof Hao-Wen Sim, Medical Oncologist, The Kinghorn Cancer Centre and Chris O’Brien Lifehouse, NSW
- Megan Trevethan, Clinical Specialist Occupational Therapy – Cancer and Lymphoedema Services, Princess Alexandra Hospital, QLD
- Chris Twyford, Cancer Specialist Nurse, Canberra Health Services, Cancer and Ambulatory Support, ACT
- Dr Adam Wells, Clinical Academic Consultant Neurosurgeon, The University of Adelaide, Royal Adelaide Hospital, SA
What is a brain tumour?
A brain or spinal cord tumour starts when abnormal cells grow and form a mass or lump. The tumour may be benign or malignant, but both types can be serious and may need urgent treatment.
Brain and spinal cord tumours are also called central nervous system or CNS tumours.
How are brain tumours classified?
Brain tumours are often classified as benign or malignant. What it means to have a benign or malignant brain tumour is usually different to what it may mean to have one in another part of the body.
Benign tumours
Many benign brain tumours grow slowly and are less likely to spread or grow back (if all of the tumour can be successfully removed). But a benign tumour may still affect how the brain works.
This can be life threatening and need urgent treatment. Sometimes a benign tumour can change over time and become malignant or more aggressive.
Malignant tumours
A malignant brain tumour may be called brain cancer. Some malignant brain tumours can grow relatively slowly, while others grow rapidly.
They are considered life-threatening because they may grow larger, spread within the brain or to the spinal cord, or come back after initial treatment.
Primary cancer
A cancer that starts in the brain is called primary brain cancer. It may spread to other parts of the nervous system.
Unlike other malignant tumours that have the potential to spread throughout the body, primary brain cancers usually do not spread outside the brain and spinal cord.
Secondary cancer
Sometimes cancer starts in another part of the body and then travels through the bloodstream or lymphatic system to the brain. This is known as a secondary cancer or metastasis.
The cancers most likely to spread to the brain are:
A metastasis keeps the name of the original cancer. For example, bowel cancer that has spread to the brain is still called metastatic bowel cancer, even though the person may be having symptoms because cancer is in the brain.
Get support
Having a brain tumour is stressful and upsetting. Experienced counsellors, psychologists or psychiatrists can offer coping strategies and ways to manage any mood swings or behavioural changes.
Call Cancer Council 13 11 20 for information or support.
Contact cancer support
The brain and spinal cord
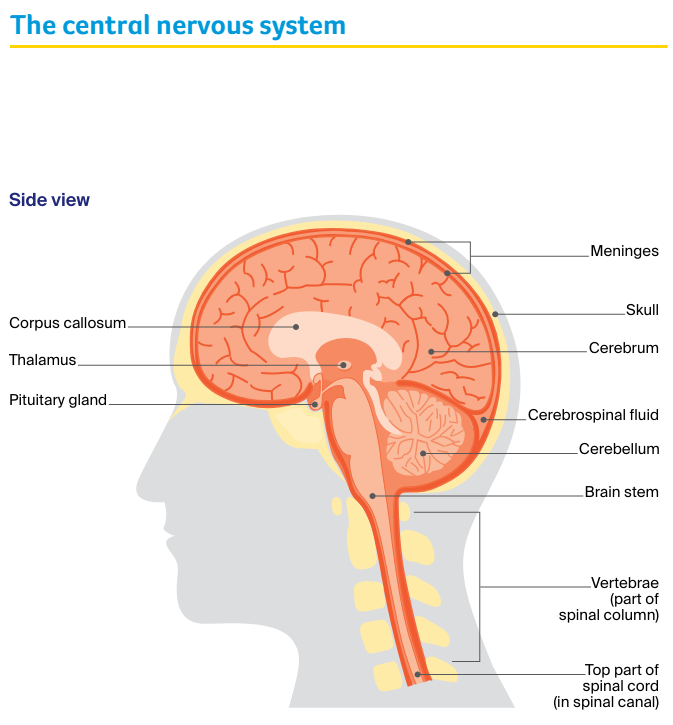
The brain and spinal cord make up the central nervous system (CNS). This CNS controls how the mind and body works.
- The brain – receives and interprets information carried to it by nerves from the sensory organs that control taste, smell, touch, sight and hearing. It also sends messages through nerves to the muscles and organs. The brain controls arm and leg movement and sensations, memory and other thinking skills, personality and behaviour, and balance and coordination. The main parts of the brain are the cerebrum, the cerebellum and the brain stem.
- Spinal cord – extends from the brain stem to the lower back. It is made up of nerve tissue that connects the brain to all parts of the body through a network of nerves called the peripheral nervous system. The spinal cord lies in the spinal canal, protected by a series of bones (vertebrae) called the spinal column.
- Meninges – thin layers of protective tissue (membranes) that cover both the brain and spinal cord.
- Cerebrospinal fluid (CSF) – found inside the skull and spinal column, CSF surrounds the brain and spinal cord and protects them from injury.
- Pituitary gland – found at the base of the brain, the pituitary gland is about the size of a pea. It makes chemical messengers (hormones) and releases them into the blood. These hormones control many body functions, including growth, fertility, metabolism and development.
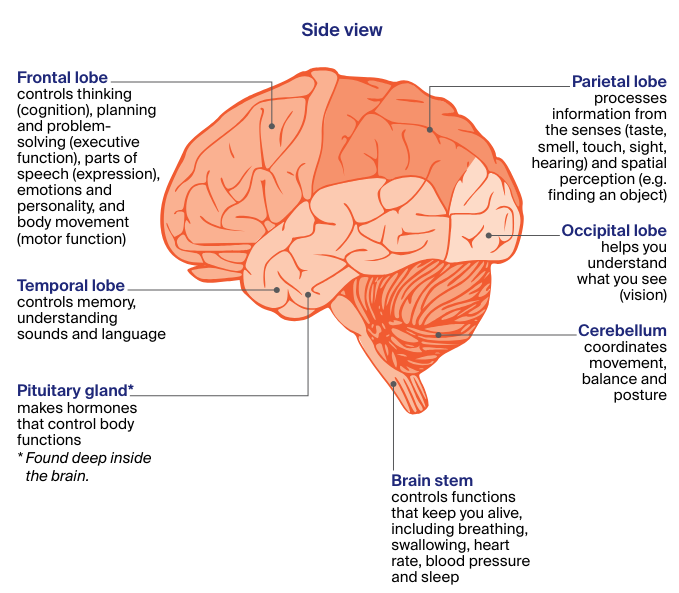
The parts of the brain and their functions
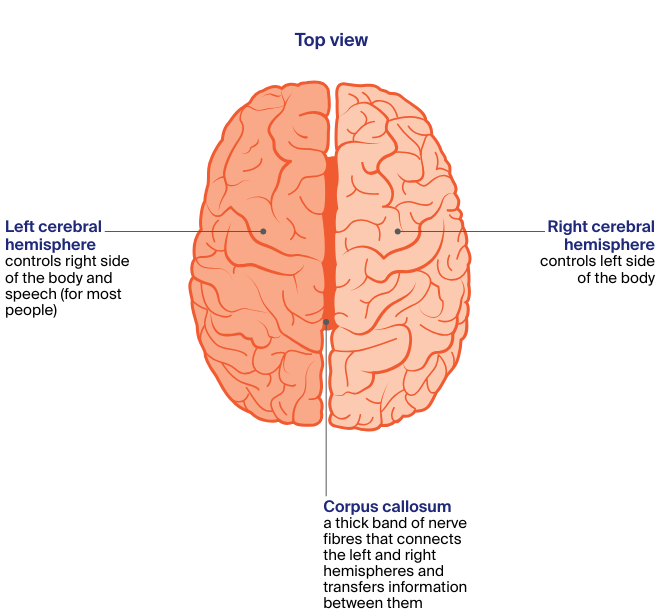
The largest part of the brain is the cerebrum. It is divided into two halves called hemispheres. Each hemisphere is divided into four main areas, called the:
- frontal
- parietal
- occipital, and
- temporal lobes.
The other main parts of the brain are the cerebellum and the brain stem. The cerebellum is found at the back of the head. The brain stem connects the brain to the spinal cord. Each part of the brain controls different bodily functions.
Your guide to best cancer care
A lot can happen in a hurry when you’re diagnosed with cancer. The guide to best cancer care for brain tumours (high grade glioma) can help you make sense of what should happen.
It will help you with what questions to ask your health professionals to make sure you receive the best care at every step.
Read the guide
Types of brain tumours
The brain is made up of different tissues and cells, which can develop into different types of tumours. There are more than 40 types of primary brain and spinal cord tumours. They can start in any part of the brain or spinal cord.
Tumours are grouped together based on the type of cell they start in and how the cells are likely to behave (based on their genetic make-up).
Glioma tumours
This is the most common type of brain tumour. Gliomas are tumours that start in the glial (neuroglia) cells of the brain. They include:
- astrocytoma – starts in glial cells called astrocytes, may be benign or malignant
- glioblastoma – a type of malignant astrocytoma that makes up more than half of all gliomas, common in both adults and children, and may develop from a slow-growing astrocytoma
- oligodendroglioma – starts in glial cells called oligodendrocytes, more common in younger adults, malignant but may be slow or fast growing
- ependymoma – starts in glial cells called ependymal cells, more common in children than adults, and may be benign or malignant
Non-glioma tumours
These tumours start in other types of cells found in the brain.
- meningioma – most common primary brain tumour that starts in the membranes (meninges) covering the brain and spinal cord, usually benign and slow growing
- medulloblastoma – malignant tumour that starts in the cerebellum, more common in children and rarer in adults
- pituitary tumour – starts in the pituitary gland, usually benign
- schwannoma – starts in Schwann cells which surround nerves in the brain and spinal cord, usually benign, includes vestibular schwannomas (sometimes called acoustic neuromas).
How common are brain tumours?
Every year an estimated 1900 malignant brain tumours are diagnosed in Australia. They are more common in men than women.
Malignant brain tumours can affect people of any age. About 110 children (aged 0–14) are diagnosed with a malignant brain tumour each year.
Benign brain and spinal cord tumours are more common than malignant tumours. The risk of being diagnosed with a brain tumour increases with age.
More about brain tumour statistics and trends
Risk factors
The cause of most brain and spinal cord tumours is unknown. As we get older the risk of developing many cancers, including brain cancer, increases. Other things known to increase a person’s risk include:
- Family history – it’s rare for brain tumours to run in families, though some people inherit a gene change from their parent that increases their risk. For example, a genetic condition called neurofibromatosis can lead to mostly benign tumours of the brain and spinal cord. Having a parent, sibling or child with a primary brain tumour may sometimes mean an increase in risk.
- Radiation therapy – people who have had radiation therapy to the head, particularly for childhood leukaemia, may have a slightly higher risk of brain tumours, such as meningioma, many years later.
- Chemical exposure – a chemical called vinyl chloride, some pesticides, and working in rubber manufacturing and petroleum refining have been linked with brain tumours.
- Overweight and obesity – a small number of meningioma brain tumours are thought to be linked to high body weight or obesity.
Mobile phones and microwave ovens
Research has not shown that mobile phone use causes brain cancer, but studies continue into any long-term effects. If you are worried, use a hands-free headset, limit time on your phone, or use messaging.
There is no evidence that microwave ovens in good condition release electromagnetic radiation at levels that are harmful to people.
Brain tumours in children
Brain tumours in children often form in different parts of the brain to adults, and may have different treatments and outlook.
Children are more likely to develop gliomas and medulloblastomas – and tumours in the lower or back part of the brain, which control sleep/wake functions, movement and coordination.
In general, children diagnosed with a malignant tumour will have a better outlook than adults. In many children, treatment will cause signs of the cancer to improve.
Because a child’s nervous system is still developing, some children may have physical, behavioural or learning difficulties due to the tumour and/or treatment. These might not show up for several years.
Treatment and support
Doctors who specialise in treating children with brain and spinal cord tumours are called paediatric oncologists. After 16 years of age, some teenagers may have treatment in an adult ward. Or they may be looked after by an adolescent and young adult multidisciplinary team.
Some hospitals have music, play or art therapists, to help children cope with the side effects of treatment. Most hospitals have occupational therapists, physiotherapists and social workers, and some may have a child life therapist.
Talk to your child’s medical team about treatment options, what to expect and your concerns. The hospital social worker can offer practical and emotional support, and suggest support services.
Cancer Hub can link you to organisations that support families, young adults and children affected by cancer – including Canteen, Camp Quality and Redkite.
Symptoms
Symptoms you may experience depend on where the tumour is, its size and how slowly or quickly it is growing. Symptoms can develop suddenly (in days or weeks) or over time (months or years).
Many symptoms are the same as other conditions, but see your doctor about any new, persistent or worsening symptoms.
Brain tumours can increase pressure inside the skull (intracranial pressure). Pressure can build up because the tumour is taking up too much space, is causing brain swelling or is blocking the flow of cerebrospinal fluid around the brain.
This increased pressure can lead to symptoms such as:
- headaches – often worse when you wake up
- nausea and vomiting – often worse in the morning or after changing position (e.g. moving from sitting to standing)
- confusion and irritability
- blurred or double vision
- seizures (fits) – some jerking or twitching of your hands, arms or legs, or affect the whole body
- weakness in parts of the body
- poor coordination
- drowsiness or loss of consciousness
- difficulty speaking or finding the right words.
Common tumour symptoms
The symptoms you experience will depend on where the tumour is in the brain or spinal cord.
Frontal lobe
- difficulty with planning or organising activities
- changes in behaviour, personality and social skills
- depression or mood swings
- weakness in part of the face, or on one side of the body
- difficulty walking
- loss of sense of smell
- problems with seeing or speaking
- trouble finding the right word
Temporal lobe
- forgetting events and conversations
- difficulty understanding what is said to you or recognising sounds
- trouble learning and remembering new information
- seizures with strange feelings, smells or deja vu
Pituitary gland (found deep inside the brain)
- headaches
- loss of vision (often side or peripheral vision)
- nausea or vomiting
- erection problems
- less interest in sex
- thyroid and other hormone changes
Brain stem
- coordination problems
- difficulty swallowing or speaking
- double vision
- weakness and numbness in part of the face
- weakness in the arms or legs
- fatigue
- changes to sleep/wake patterns
Parietal lobe
- problems with reading or writing
- loss of feeling in part of the body
- difficulty telling left from right
- difficulty locating objects around you
Occipital lobe and meninges
- loss of all or some vision
- headaches
- vomiting
- weakness in the arms or legs
- personality changes or confusion
Cerebellum
- coordination and balance problems
- uncontrolled eye movement
- stiff neck
- dizziness
- difficulty speaking (staccato speech)
Spinal cord
- back and neck pain
- numbness or tingling in the arms or legs
- change to muscle tone in the arms or legs
- clumsiness or difficulty walking
- loss of bowel or bladder control (incontinence)
- change in the feeling in the genital or anal area or erection problems
Nerve and other tumours
Symptoms of tumours starting in the brain’s nerves (cranial nerves) depend on the affected nerve. The most common nerve tumours are vestibular schwannomas (acoustic neuromas). They can cause hearing loss, dizziness and balance issues.
Vestibular schwannomas are usually benign. Tumours of the pineal gland (deep within the brain) are very rare and usually classified as neuroendocrine tumours.
Health professionals you'll see
Your general practitioner (GP) or another doctor will arrange the first tests to assess your symptoms.
If these tests do not rule out a tumour, you will usually be referred to a specialist, such as a neurosurgeon or neurologist, who will examine you and arrange further tests.
Often these will be discussed with other health professionals at what is known as a multidisciplinary team (MDT) meeting.
During and after treatment you will see a range of health professionals, which may include a medical oncologist, neuropathologist, rehabilitation specialist and exercise physiologist, who specialise in different aspects of your care.
Question checklist
Asking your doctor questions will help you make an informed choice. You may want to include some of the questions below in your own list.
Diagnosis
- What type of brain or spinal cord tumour do I have?
- Where is the tumour? How extensive is the tumour? How fast is it growing?
- Will a multidisciplinary team be involved in my care?
- Are there clinical guidelines for this type of cancer?
Treatment
- What treatment do you recommend? What is the aim of the treatment?
- Are there other treatment choices for me? If not, why not?
- If I don’t have the treatment, what should I expect?
- How long do I have to make a decision?
- I’m thinking of getting a second opinion. Can you recommend anyone?
- How long will treatment take? Will I have to stay in hospital?
- Are there any out-of-pocket expenses not covered by Medicare or my private health cover? Can the costs be reduced if I can’t afford it?
- How will we know if the treatment is working?
- Are there any clinical trials or research studies I could join?
Side effects
- What are the risks and possible side effects of each treatment?
- Will I have a lot of pain? What will be done about this?
- Can I work, drive and do my normal activities while having treatment?
- Will the treatment affect my sex life and fertility?
- Should I change my diet or physical activity during or after treatment?
- Are there any complementary therapies that might help me?
- How can I access rehabilitation services?
- Who do I contact if I have concerns about side effects?
After treatment
- How often will I need check-ups after treatment?
- If the tumour returns, how will I know? What treatments could I have?
