Page last updated: April 2025
The information on this webpage was adapted from Understanding Bowel Cancer - A guide for people with cancer, their families and friends (2025 edition). This webpage was last updated in April 2025.
Expert content reviewers:
This information was developed based on Australian and international clinical practice guidelines, and with the help of a range of health professionals and people affected by bowel cancer:
- Prof Alexander Heriot, Colorectal Surgeon and Director Cancer Surgery, Peter MacCallum Cancer Centre, Director, Lower GI Tumour Stream, Victorian Comprehensive Cancer Centre, VIC
- Dr Cameron Bell, Gastroenterologist, Royal North Shore Hospital, NSW
- Graham Borgas, Consumer
- Prof Michael Bourke, Director of Gastrointestinal Endoscopy, Westmead Hospital, The University of Sydney, NSW
- Laura Carman, 13 11 20 Consultant, Cancer Council Victoria, VIC
- Amanda Connolly, Specialist Bowel Care Nurse, Icon Cancer Centre Windsor Gardens, SA
- A/Prof Melissa Eastgate, Operations Director, Cancer Care Services, Royal Brisbane and Women’s Hospital, QLD
- Anne Marie Lyons, Stomal Therapy Nurse, Concord Repatriation General Hospital and NSW Stoma Ltd, NSW
- Lisa Nicholson, Manager Bowel Care Services, Bowel Cancer Australia, NSW
- Stefanie Simnadis, Clinical Dietitian, St John of God Subiaco Hospital, WA
- Rafi Sharif, Consumer
- Dr Kirsten van Gysen, Radiation Oncologist, The Nepean Cancer and Wellness Centre, NSW
- Sarah Williams, Clinical Nurse Consultant, Lower GI, Peter MacCallum Cancer Centre, VIC
What is bowel cancer?
Bowel cancer (also called colorectal cancer) is cancer in any part of the large bowel (colon or rectum). It may also be called colon cancer or rectal cancer, depending on where in the bowel it is.
The cancer starts in the lining of the inner bowel wall (called the mucosa). It usually develops from small growths called polyps. Most polyps are harmless (benign), but some may turn into cancer.
Removing polyps during a colonoscopy reduces the risk of bowel cancer. If untreated, bowel cancer can grow into the deeper layers of the bowel wall. It can also spread to the lymph nodes.
If the cancer advances further, it can spread to other organs, such as the liver or the lungs.
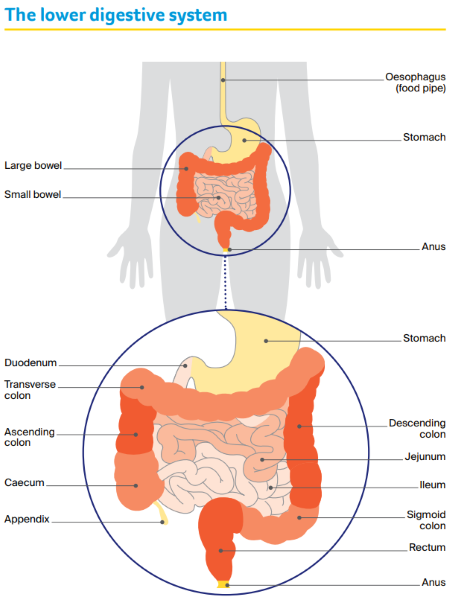
The bowel
The small bowel (also called small intestine)
This is a long tube (4–6 metres) that absorbs nutrients from food. It is longer and narrower than the large bowel. It has three parts:
- duodenum – top section; receives broken-down food from stomach
- jejunum – middle section
- ileum – lower, longest section; moves waste to large bowel.
See Understanding small bowel cancer for more information.
The large bowel (also called large intestine or colon)
About 1.5 metres long, this tube absorbs water and salts, and turns what is left into solid waste (faeces, stools or poo). The large bowel has three parts:
- caecum – looks like a pouch; it receives waste from the small bowel; the appendix is attached to the caecum (see Understanding appendix cancer and PMP for more information)
- colon – main, longest section of the large bowel, has four parts: ascending colon, transverse colon, descending colon and sigmoid colon
- rectum – the last 15–20 centimetres of the large bowel.
This page is only about cancer of the large bowel.
The anus
This is the opening at the end of the large bowel. During a bowel movement, the anal muscles relax to release faeces (poo). See Understanding anal cancer for more information.
Your guide to best cancer care
A lot can happen in a hurry when you’re diagnosed with cancer.
The guide to best cancer care for bowel cancer can help you make sense of what should happen. It will help you with what questions to ask your health professionals to make sure you receive the best care at every step.
Read the guide
How common is bowel cancer?
Bowel cancer is the 4th most common cancer in Australia. Each year, about 15,500 Australians are diagnosed with bowel cancer. It is more common in people over 50, but it can happen at any age.
The number of adults under 50 with bowel cancer is increasing, with research yet to give a clear reason for this.
Learn more about bowel cancer statistics and trends
Less common types of bowel cancer
Most bowel cancers are adenocarcinomas, which start in the tissue lining the large bowel. Rarely, other less common types of cancer can also affect the bowel. These include:
- lymphomas
- squamous cell carcinomas
- neuroendocrine tumours, and
- gastrointestinal stromal tumours.
Cancer can also start in the small bowel (called small bowel cancer or small intestine cancer), or in the appendix, but this is rare. These cancers are not included in this booklet, and may have different treatment.
Learn more about small bowel cancer
Learn more about appendix cancer and PMP
What are the symptoms?
Some people have no symptoms and the cancer is found through screening. However, many people with bowel cancer experience some of the symptoms listed below.
Other conditions can also cause the same symptoms, including irritable bowel syndrome (IBS), diverticulitis (inflammation of pouches in the bowel), inflammatory bowel disease, haemorrhoids, or an anal fissure (cracks in the skin lining the anus).
Having some of the symptoms on this list does not mean that you definitely have bowel cancer. Talk to your doctor if you have any of these symptoms, especially if they are ongoing, get worse, or if there is any bleeding:
- blood in or on faeces (poo) or on the toilet paper; this might be bright red or make the poo look dark brown or black
- a persistent or unexplained change in bowel habits, such as diarrhoea or loose stools, constipation or smaller, more frequent bowel movements
- a change in the look of faeces (e.g. narrower or with mucus)
- a feeling of fullness or bloating in the abdomen (belly) or a strange sensation in the rectum, often during a bowel movement
- feeling that the bowel hasn’t emptied completely after you have done a poo
- losing weight without trying to
- rectal or anal pain
- a lump in the rectum or anus
- abdominal pain or swelling
- weakness or fatigue, dizziness or breathlessness
- a low red blood cell count (anaemia or iron deficiency)
- a blockage in the bowel.
Bowel screening
The National Bowel Cancer Screening Program is a free test available to Australians aged over 45. If you have a positive test, you will need a colonoscopy
Learn more
What are the risk factors?
Anything that can increase your risk of cancer is called a risk factor. For bowel cancer, these include:
- older age – bowel cancer is more common in people over 50, but the number of younger people being diagnosed is increasing
- polyps – most polyps can become bowel cancer; having a large number of polyps in the bowel is a strong risk factor
- dietary factors – a diet that is low in fibre, fruit, vegetables and wholegrains, and high in red and processed meats such as salami, ham and bacon
- smoking – increases your risk of bowel cancer and bowel polyps
- drinking alcohol – the less alcohol you drink, the lower your risk. If you choose to drink, follow the Australian Alcohol Guidelines
- body weight – being above a healthy weight
- physical inactivity – not moving your body enough. Be active on most days and minimise long periods of sitting
- strong family history – a small number of bowel cancers and types of polyps run in families
- other bowel diseases – inflammatory bowel diseases, such as Crohn’s disease or ulcerative colitis, significantly increase risk, particularly if you have had the disease for more than 10 years (IBS does not increase your risk)
- other cancers – people who have had bowel cancer are more likely to develop a second bowel cancer; some people who have had ovarian cancer or cancer of the uterus, or who have had radiation treatment to the abdomen/pelvis, may also have an increased risk of bowel cancer
- type 2 diabetes – this may increase your risk of bowel cancer
- rare genetic disorders – some bowel cancers are linked to an inherited gene or condition (e.g. cystic fibrosis).
Can bowel cancer run in families?
Sometimes bowel cancer runs in families. The risk of developing bowel cancer may be higher if one or more of your close family members (a parent, brother or sister) has had bowel cancer.
The risk is higher if they were diagnosed before the age of 50, or if two or more close relatives have had bowel cancer.
A family history of some other cancers, such as cancer of the uterus (endometrial cancer), may also increase the risk (see Lynch syndrome, below).
Some people have an inherited faulty gene that increases their risk of developing bowel cancer. These faulty genes are responsible for a small number of bowel cancers in the population.
There are two main genetic conditions that occur in some families:
Lynch syndrome
Less than 5% of bowel cancers are linked to Lynch syndrome, which causes a fault in the gene that helps repair a cell’s DNA.
People with Lynch syndrome have an increased risk of developing bowel cancer, cancer of the uterus, and other cancers such as kidney, bladder and ovarian. Bowel cancer may also happen at a younger age than usual.
Learn more
Familial adenomatous polyposis (FAP)
This condition is linked to about 1% of bowel cancers. It causes hundreds of polyps to form in the bowel. If these polyps are not removed, they may become cancerous.
If you have a family history, talk to your doctor about regular check-ups or ask for a referral to a family cancer clinic.
Which health professionals will I see?
Your general practitioner (GP) will arrange the first tests to assess your symptoms, or further tests if you have had a positive screening test.
If these tests do not rule out cancer, you will usually be referred to a specialist, such as a gastroenterologist or colorectal surgeon.
The specialist will arrange further tests. If bowel cancer is diagnosed, the specialist will consider treatment options. Often these will be discussed with other health professionals at what is known as a multidisciplinary team (MDT) meeting.
During and after treatment, you may see a range of health professionals who specialise in different aspects of your care.
